"The incorporation of NGI into the BCR disease state definition necessitates a consensus within the medical community," write Spyridon P. Basourakos, MD, and Jack R. Andrews, MD.
Basourakos is a urologic oncology fellow at Mayo Clinic in Rochester, Minnesota. Andrews is a urologic oncologist with Mayo Clinic in Phoenix, Arizona.
Prostate cancer is the most frequently diagnosed solid tumor in men, accounting for 30% of all new cancer cases in men.1 When dealing with aggressive localized forms of the disease, patients are presented with various
treatment options, including radical prostatectomy and external beam radiation therapy. However, within a decade following primary treatment, 20% to 50% of these patients experience biochemical recurrence (BCR), indicating either a local resurgence of the disease or the presence of metastases, both of which significantly affect survival rates.2,3 Consequently, crafting a customized treatment approach is essential. The imaging evaluation of patients with suspected BCR is crucial, providing vital information needed by a multidisciplinary health care team—including medical oncologists, radiation oncologists, radiologists, pathologists, and urologists—to make informed clinical decisions. In this article, we explore both conventional and next-generation imaging (NGI) techniques available for identifying recurrent prostate cancer.
Conventional imaging methods such as CT scans, MRI, and technetium-99m bone scintigraphy have long served in detecting cancer progression in the BCR setting.4 Yet these techniques often fall short in effectively detecting low-volume metastatic or locally recurrent disease, especially at low levels of prostate-specific antigen (PSA) when salvage therapy would be most effective.5 It has been shown that the likelihood of positive findings in bone scans and CT scans is less than 5% and 15%, respectively, when performed in men with recurrent disease and PSA levels under 10 ng/mL.6-8 Therefore, although traditional imaging remains a part of the guidelines for BCR workup, the medical community is increasingly leaning toward NGI techniques that provide greater diagnostic accuracy.
In recent years, PET has emerged as a new imaging modality. This noninvasive, molecular imaging technique utilizes various radiolabeled tracers—comprising a radionuclide attached to a biologically active molecule—specifically designed to target particular receptors and thus pinpoint the location of disease. Research has shown that PET’s ability to integrate functional and spatial-anatomical information offers superior diagnostic capabilities compared to conventional imaging for patients with BCR.9 The advent of PET combined with CT (PET-CT) or MRI, particularly with the introduction of tracers beyond F-18 fluorodeoxyglucose, has significantly advanced the staging of recurrent or metastatic prostate cancer, even in cases with small-volume disease. As of now, the FDA has approved 5 PET tracers for evaluating patients with BCR of prostate cancer: Ga-68 PSMA-11 (PSMA-HBED-CC), F-18 piflufolastat (DCFPyL), C-11 choline, F-18 fluciclovine, and F-18 sodium fluoride.10 For practical considerations, we will primarily focus our discussion on C-11 choline and PSMA (prostate-specific membrane antigen) PET radiotracers.
Choline plays a crucial role in the synthesis of phospholipids for all cellular membranes and, therefore, prostate cancer cells demonstrate increased uptake when C-11 choline tracer is used. Studies suggest that a PSA level ranging from 1 ng/mL to 2 ng/mL is the most effective range for choline PET to diagnose BCR. In a study of 358 patients with BCR undergoing 11C-choline PET-CT scans, the likelihood of positive scan results escalated with rising PSA levels: 19% for PSA levels between 0.2 ng/mL and 1 ng/mL, 46% for those between 1 ng/mL and 3 ng/mL, and 82% for levels exceeding 3 ng/mL.11 Graziani et al evaluated the role of C-11 choline PET as a staging tool after BCR on more than 4400 men and showed that the PSA level was the main predictor of a positive scan with 1.16 ng/mL as the optimal cutoff value. In the majority of those positive scans, metastatic disease was identified while still treatable with salvage therapies.12 Meta-analyses indicate that 11C-choline PET-CT scans are highly accurate in identifying lymph node metastasis and distant lesions. However, the efficacy in detecting local recurrences remains uncertain, primarily due to significant variability across different studies. Meta-analyses indicate that 11C-choline PET-CT scans are highly accurate in identifying lymph node metastasis and distant lesions. However, the efficacy in detecting local recurrences remains uncertain, primarily due to significant variability across different studies.13 One of the major constraints of C-11 choline use is its short half-life of 20 minutes, requiring access to a nearby cyclotron-radiochemistry facility. The latter poses significant challenges for widespread adoption across facilities.
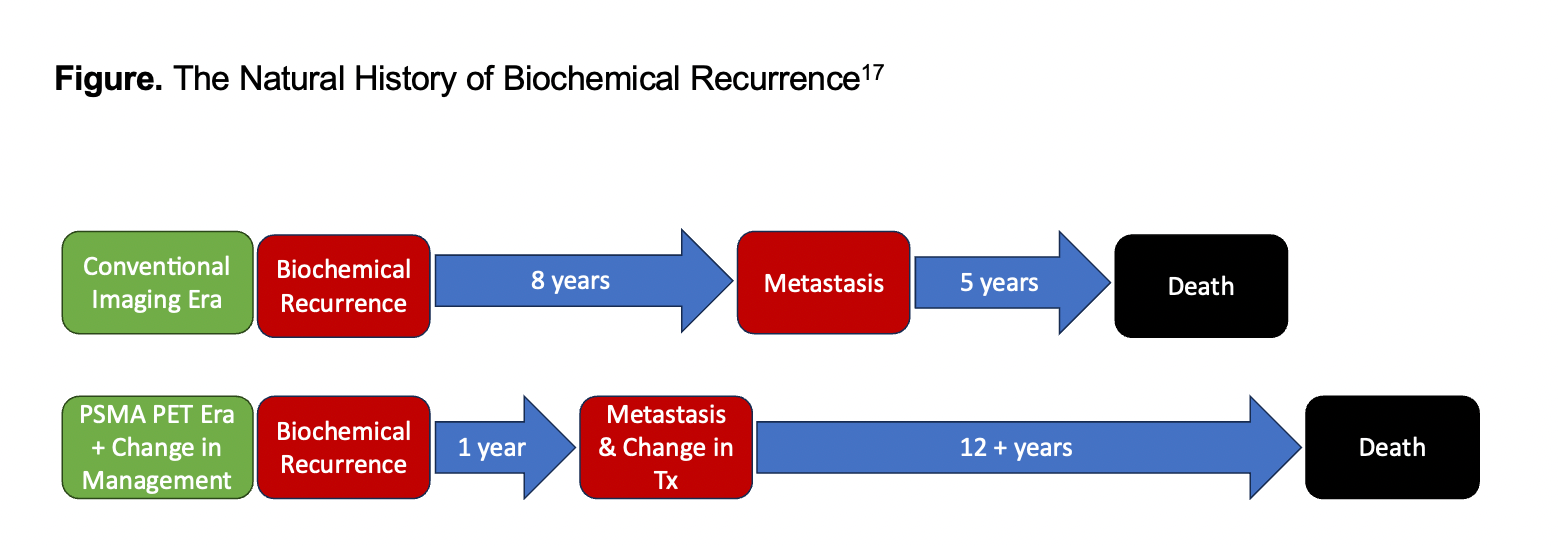
In cases of BCR, the National Comprehensive Cancer Network guidelines now prioritize PSMA PET-CT as the imaging method of choice due to its superior sensitivity and specificity in detecting micrometastases, surpassing conventional imaging methods. The detection capabilities of Ga-68 PSMA-11 for biochemically recurrent prostate cancer have been reported with positive predictive values ranging between 84% and 92%.14 Similarly, the tracers 18F-DCFPyL and rhPSMA-7.3 have shown positive predictive values of 89% and 92%, respectively.15,16 Despite these advancements in PSMA imaging interpretation, clinical trials are needed to explore changes in management for PSMA-avid lesions in the setting of negative conventional imaging. Research by Pound et al has highlighted that the median time from untreated BCR to the detection of metastasis via conventional imaging was 8 years, with an additional median lifespan of 5 years post development of metastatic disease.17 This underscores the importance of identifying metastatic disease earlier and investigating new treatment approaches to extend survival (Figure17). Although PSMA PET-CT can enhance disease staging through stage migration, its potential to improve survival critically depends on the effective use of early radiographic metastasis diagnoses. With the increasing use of PSMA PET-CT, the role of metastasis-directed therapies is anticipated to grow correspondingly.

NGI with PET is revolutionizing the assessment and management of BCR in prostate cancer. The advent of NGI, bolstered by clinical evaluations of various novel radiotracers, is steering a paradigm shift away from conventional imaging methods in facilities equipped with these advanced technologies. This shift is primarily due to NGI’s enhanced sensitivity in detecting recurrent disease at lower PSA levels compared with traditional methods, thereby broadening treatment options and paving the way for novel interventional strategies aimed at improving patient outcomes. However, the incorporation of NGI into the BCR disease state definition necessitates a consensus within the medical community. This consensus is vital for refining the BCR definition to accurately reflect the diagnostic advancements brought about by NGI. Such a revised definition would acknowledge NGI’s capacity to detect recurrences at lower PSA levels and improve staging, which has significant implications for treatment decision-making and introduces opportunities for innovative treatments that could potentially enhance patient care outcomes.